Contact Us
CiiS Lab
Johns Hopkins University
112 Hackerman Hall
3400 N. Charles Street
Baltimore, MD 21218
Directions
Lab Director
Russell Taylor
127 Hackerman Hall
rht@jhu.edu

Last updated: 5/10/2013 by pwilken3
In many cases of hearing loss, especially those involving damage to the sensory hair cells of the cochlea, hearing can be restored by way of a cochlear implant. These devices are arrays of electrodes that are curled inside the cochlea, and transmit sound sent by an external receiver into electrical signals that are sent to the brain. The implantation of the electrode array is a difficult procedure even for highly trained surgeons due to low visibility, the precision required, and the small scale of the force that can cause damage to the cochlea. In order to make this procedure safer and more repeatable, we propose a system that uses a tremor-cancelling robot that guides the implant along the axis of the cochlea to the point of insertion. Virtual fixtures are enacted based on imaging that constrain the motion of the robot to the center axis of the cochlea, guiding the implant to the ideal insertion point. This increases the chance of success for the operation, as well as minimizing the chance of cochlear damage.
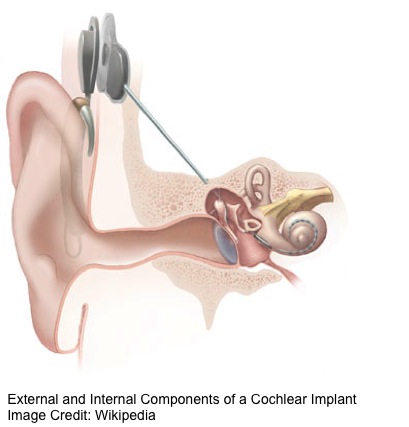
In order to access the cochlea, the surgeon must first perform a mastoidectomy and cochleostomy. The mastoidectomy machines the flesh (mastoid cells) around the cochlea, and the cochleostomy drills a hole into the temporal bone. Once this is complete the round window, the most direct entrance to the cochlea, is accessible. The surgeon then inserts the implant until the desired position is reached. This is typically just before the basal turn, which is the first turn in the spiral of the cochlea. This location is communicated by way of a marker on the implant itself. Once this marker reaches the site of the cochleostomy, the implant should be at the proper depth. The surgeon then grips the stylet, a wire that keeps the implant straight, and continues to push the electrode array. Because the electrode array is naturally curved, removing it from the stylet causes it to curve into the spiral of the cochlea and the insertion is then complete.

<html><center></html><fs x-small>Cochlear Implant inserted to Ideal Insertion Point in Cochlear Phantom</fs><html></center></html>
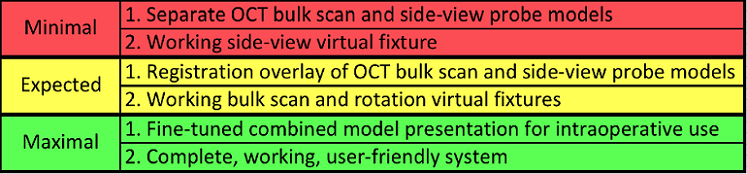
Aims:
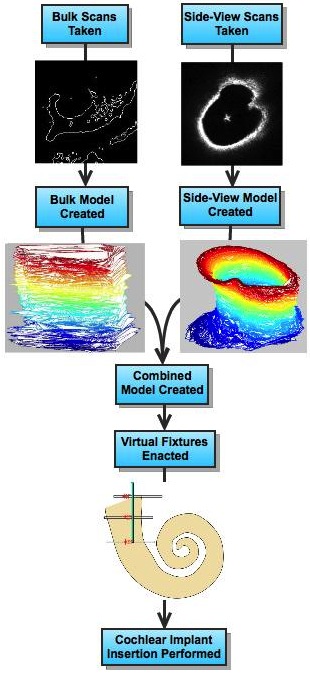
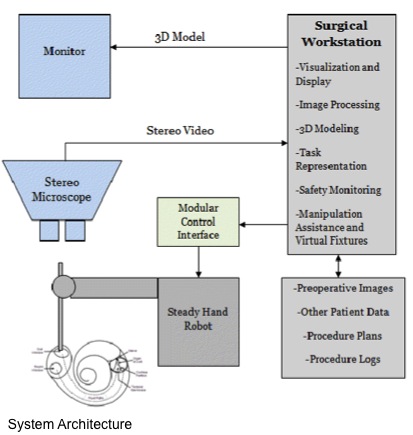
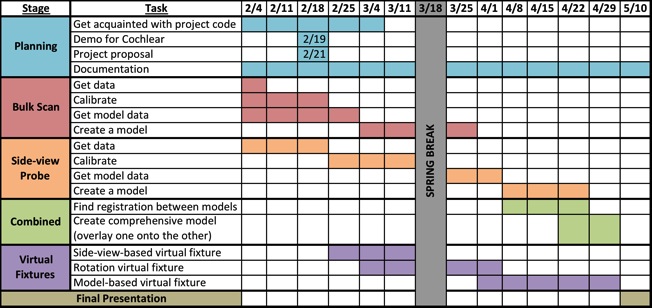
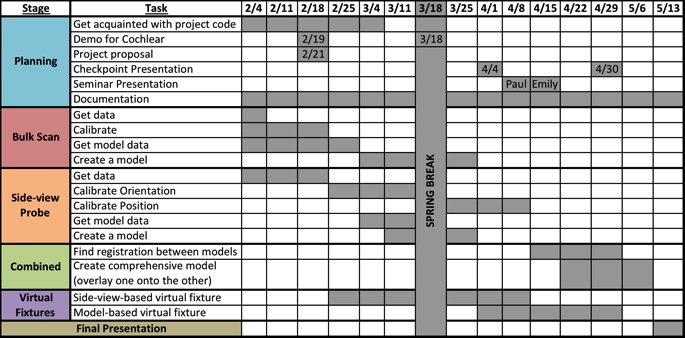
<html><center></html><fs x-small>Project Workflow</fs><html></center></html>
This project is significant because cochlear implant insertion is a difficult procedure that has widespread use. As of December 2010, 219,000 people worldwide use cochlear implants [8]. The market for cochlear implants is large, and several companies are working to develop cochlear implants that are easier to insert. Cochlear is a company that is working closely with ERC CISST to develop implants suited to a robotic system for this insertion, and their investment of time, effort, and resources showcases the potential effect this system can have once implemented. The methods used in this project also have potentials applications to other surgical procedures, as they increase the overall safety of the surgery by constraining the movement of the robot.
The steady-hand robot is a robotic arm to which the side-view probe, bulk OCT scanner, and implant-holding tool can be mounted. It uses tremor-reduction to eliminate the hand tremors surgeons train to reduce, but can never completely remove. Even these slight hand tremors can cause significant damage to the cochlea, and so this is an important piece of the system. The robot is also able to enact virtual fixtures, which are constraints on the motion of the robot in its environment. The virtual fixtures we will use are discussed in more detail below.
Side-viewing Probe Imaging
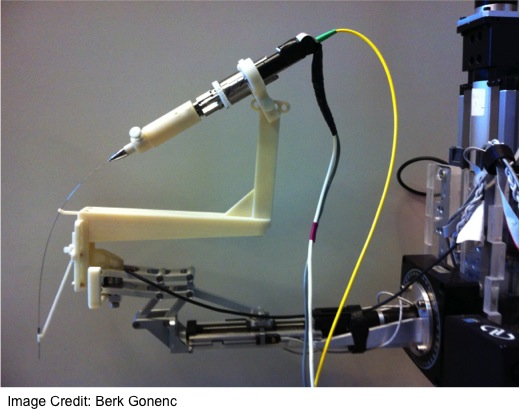
<html><center></html><fs x-small>Side-view Probe Setup</fs><html></center></html>
A probe has been developed that uses an angled fiber to capture OCT A-scans out of a window drilled into its side. It can be mounted to a motor that turns the sideview probe, enabling it to create B-scans out of the A-scans it receives and create a contour that shows a 360 degree view of its surroundings, up to 5 mm. When inserted into the cochlea, it can give contours at several depths, which can then be stitched together into a model of the cochlea. These contours are also useful for virtual fixtures, which is discussed below.
Bulk Scan Imaging
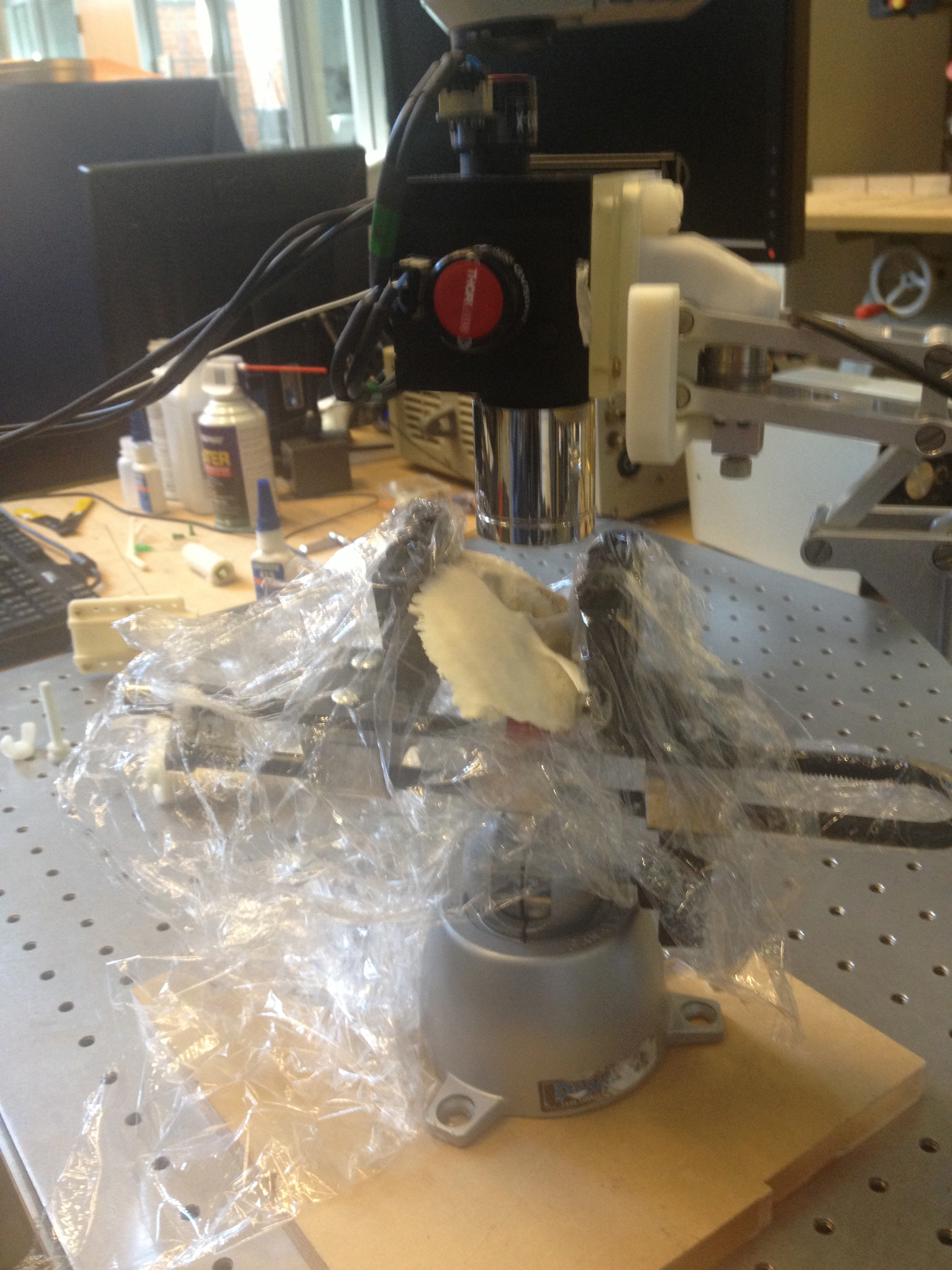
<html><center></html><fs x-small>Bulk Scanner Setup</fs><html></center></html>
An OCT bulk scanner has been constructed that can create a 5 mm x 5 mm x 5 mm volume. It takes several A-scans until a row is complete, and then takes A-scans for the next row. This process is repeated until a cube has been populated. The size of this volume isn't sufficient to capture the entire cochlea, but several are taken and then the images are stitched together. This volume can then be turned into a surface model, which is useful for virtual fixtures.
Virtual Fixtures
We plan on implementing several virtual fixtures that will assist in inserting the implant. The first virtual fixture is halting the implant at the basal turn and capturing the axis of insertion. This virtual fixture saves the coordinates of a point identified to be the basal turn, and the orientation of the robot at the point. From then on, when the virtual fixture is enacted the robot will only be able to move the implant along that axis and halts all motion once the desired point is reached. This way, a user will be able to guide the implant along the proper axis and the stop will notify them that the proper depth has been reached. This is difficult to achieve without the virtual fixture, so it is a good first step in proving that such an insertion can be repeated reliably.
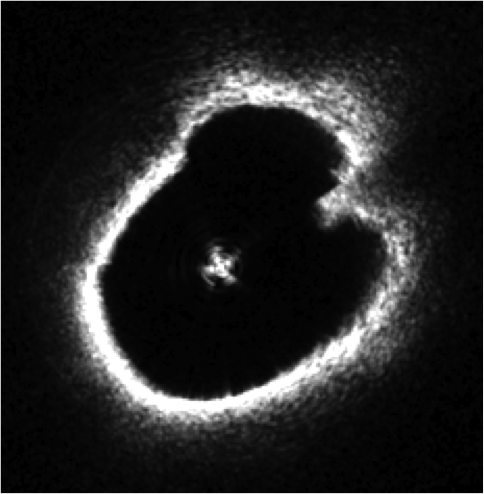
<html><center></html><fs x-small>Side-view Probe B-scan</fs><html></center></html>
A second virtual fixture involves the side-view probe's contours. These can be used to identify the center of the cochlea and location of the probe at several depths, and the virtual fixture guides the probe so that it is in the center of the cochlea at all depths. The side-view probe is currently very difficult to insert, so this virtual fixture will greatly help us get better B-scans.
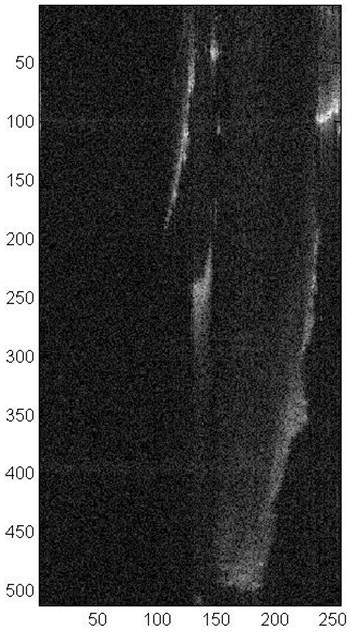
<html><center></html><fs x-small>Slice of Bulk Scan Volume</fs><html></center></html>
Another virtual fixture involves the volume obtained by the bulk OCT scanner. The model extrapolated from this volume can be used to identify the desired axis of insertion and point of insertion, which would then be used with our first virtual fixture to assist in inserting the implant. Instead of needing to insert and determine the desired location manually, it can be done automatically. This would allow us to find this point without expert guidance, which would be greatly helpful.
[1] Coulson, C. J., Reid, A. P., Proops, D. W., & Brett, P. N. (2007). ENT challenges at the small scall. The International Journal of Medical Robotics and Computer Assisted Surgery, (3), 91-96.
[2] Kapoor, A., Li, M., & Taylor, R. (2006). Constrained control for surgical assitant robots. Proceedings of the 2006 IEEE International Conference on Robotics and Automation, Orlando, Florida.
[3] Kavanaugh, K. T. (1994). Applications of image-directed robotics in otolaryngologic surgery. The Laryngoscope, (104), 283-293.
[4] Lin, J., Staecker, H., & Jafri, M. S. (2008). Optical coherence tomography imaging of the inner ear: A feasibility study with implications for cochlear implantation. Annals of Otology, Rhinology & Laryngology, 117(5), 341-346.
[5] Majdani, O., Rau, T. S., Baron, S., Eilers, H., Baier, C., Heimann, B., . . . Leinung, M. (2009). A robot-guided minimally invasive approach for cochlear implant surgery: Preliminary results of a temporal bone study. International Journal of Computer Assisted Radiology and Surgery, (4), 475-486.
[6] Pau, H. W., Lankenau, E., Just, T., Behrend, D., & Hüttmann, G. (2007). Optical coherence tomography as an orientation guide in cochlear implant surgery? Acta Oto-Laryngologica, (127), 907-913.
[7] Rau, T. S., Hussong, A., Leinung, M., Lenarz, T., & Majdani, O. (2010). Automated insertion of preformed cochlear implant electrodes: Evaluation of curling behaviour and insertion forces on an artificial cochlear model. International Journal of Computer Assisted Radiology and Surgery, (5), 173-181.
[8] Zhang, J., Wei, W., Ding, J., Roland, J. T. J., Manolidis, S., & Simaan, N. (2010). Inroads toward robot-assisted cochlear implant surgery using steerable electrode arrays. Otology & Neurotology.
Code SVN: https://svn.lcsr.jhu.edu/cochlear/
Code ZIP File: codezip.zip