Contact Us
CiiS Lab
Johns Hopkins University
112 Hackerman Hall
3400 N. Charles Street
Baltimore, MD 21218
Directions
Lab Director
Russell Taylor
127 Hackerman Hall
rht@jhu.edu

Last updated: 05/18/17
Patients that have been affected by stroke improve most in motor skills when treatment is administered within the first couple months after the incident. By introducing a user-friendly, portable, and relatively low-cost device that can record and process small forces from the fingers that are typically characteristic of severe stroke cases, early intervention and treatment of stroke becomes more practical and feasible for a larger demographic of patients.
Arguably one of the more debilitating injuries are lesions that affects the strength and control of the hands and upper limbs, which makes it difficult to perform everyday tasks including grabbing objects and interacting with computers. In the case of computer interface, stroke affected patients may not be able to target with a single finger and slide with sufficient range on a touchscreen. Some patients may not even feel the sense of touch when interacting with a tactile screen, making the act of consistent pressing difficult. Researchers at Johns Hopkins’ own Department of Neurology have recently completed a study into post-stroke recovery of the human hand, which has revealed that both strength and control in the hand generally improves the most within the first three months (or twelve weeks) of recovery. Therefore, it is key to introduce rehabilitation to the patient as early as possible to improve the chances and effectiveness of recovery, which can lead to a better quality of life for the patient.
Goals of this project include:










")
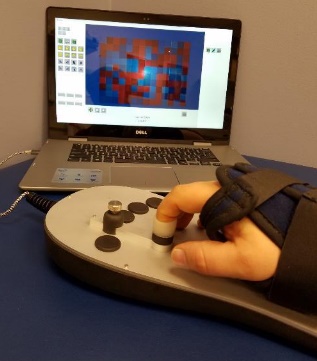
Patients will have their hand of focus fitted into an adjustable wrist brace that locks into the base of the rehab tool. The fingers of the patient will fit into up to five adjustable silicon retention cups. The base of each cup structure will contain a strain-gauge force-sensor array that can detect pressing, lifting, and lateral pressures from the patient at a high sensitivity to account for the potential weakness of the patient. The signal changes from the sensor arrays are sent to a controller board inside the tool and then to a connected computer, which processes the signal fluctuations into useful information that can be used in higher-level applications or games.
UPDATE: All needed parts have been ordered and received, so this dependency has been resolved.
UPDATE: Due to a transition in clinical study focus to a collaboration with Western University, current progress on IRB and CES approval has been put on hold until further notice. Therefore, the project has indeed shifted to a more technical focus with design being driven by techincal objectives and client needs rather than direct patient feedback.
UPDATE: Western University will deal with much of the patient selection for its own study, but this dependency may become relevant again if an American counterpart to this study is developed.
[1] K. Nagata, “Fingertip-mounted six-axis force sensor”. US Patent 6622575 B1, 7 July 1999.
[2] J. Xu, A. Haith, J. Krakauer, “Motor control of the hand before and after stroke,” Clinical Systems Neuroscience, Ed. K. Kansaku et al. Springer Japan, 2015.
[3] J. Xu, N. Ejaz, B. Hertler, M. Branscheildt, M. Widmer, A. Faria, M. Harran, J. Cortes, N. Kim, P. Celnik, T. Kitago, A. Luft, J. Krakauer and J. Diedrichsen, “Recovery of hand function after stroke: separable systems for finger strength and control,” bioRxiv, 2016.
[4] R. Pozos and J. Agraz, “Force measuring device and method”. US Patent 6673026 B2, 27 March 2000.
[5] S. Ito, H. Kawasaki, Y. Ishigure, Y. Nishimoto, T. Aoki, T. Mouri, H. Sakaeda and M. Abe, “Development of a Hand Motion Assist Robot for Rehabilitation Therapy by Patient Self-Motion Control,” in Proceedings of the 2007 IEEE 10th International Conference on Rehabilitation Robotics, Noordwijk, Netherlands, 2007.